
Notice. Since this seems to be such a common question I think I should describe my background. I have a PhD in molecular microbiology and I was once a tenured academic (professor). I now work in the biotech sector. I have published a number of peer reviewed papers in virology. If you really want to know more about me then visit my About Me page.
Like nearly everyone on the planet I am worried about COVID-19. SARS-CoV-2 (the virus that causes COVID-19) appears to be killing between 1% to 3.5% of the people we know it infects (i.e the case fatality rate) and has a R0 (i.e. how many new people each person infected goes on to infect) of between 2.5 to 3.9 or even higher.
Newer reliable serology data, such as the studies done in Switzerland and China (i.e. not Santa Clara or Los Angeles), suggests the true infection fatality rate (IFR) is around 1%. Left to run wild, this virus will kill tens of millions of people worldwide.
Many governments of the world have implemented strict population isolation protocols to try and limit the spread of the virus, but the economic cost of this is extremely high. A vaccine for COVID-19 is 12 to 18 months away (at best).
We are stuck in a diabolic situation where the only way to prevent the economy sliding into a slump deeper than the Great Depression is to consign many tens of millions of people to an early grave. Is there a way out?
SARS-Cov-2 Viral Diversity
SARS-CoV-2 like all viruses mutates (changes) overtime. Many of these genetic changes are small (single nucleotides) that are not important to the replications or transmission of the virus from person to person, but they can be used to identify the origin of the virus. DeCODE genetics for example has been testing Icelanders for COVID-19 and genome sequencing the SARS-CoV-2 strains isolated. They (and others) have found two very important pieces of information:
- More than 50% of the people infected with SARS-CoV-2 are asymptomatic or have only a mild case (i.e. they have no serious illness).
- They can identify the geographical origin of the strains by the genetic differences (mutations) between the different strains.
Furthermore, researchers in China have identified a mutant strain of SARS-CoV-2 which appears to be less pathogenic than most strains infecting people. The strain (ZJ01) had single nucleotide mutations in a key functional gene that made it less able to spread through the body. A recent pre-print paper from Singapore has described a mutant strain of SARS-CoV-2 with a 382 nucleotide deletion that was found in a cluster of patients in one of their hospitals. An even more recent paper from China found 11 of strains of SARS-CoV-2 with variation in pathogenicity in cell culture.
This data suggests a simple and testable hypothesis – there are natural strains of SARS-CoV-2 in the world that have mutated to be non-pathogenic (asymptomatic or mild), but which are still infective and will provide immunity to the more pathogenic (deadly) strains.
If we can find one of these non-pathogenic viral strains out in the wild we could give it to everyone in the world and solve our diabolic problem. This non-pathogenic (attenuated) strain would act much like the live attenuated (oral) polio vaccine.
Update. The genome sequence data collected to date has found that there are many SARS-CoV-2 strains with gene deletions.
How do we find an attenuated SARS-CoV-2 strain?
This hypothesis is worthless if we have no way of finding any of these non-pathogenic SARS-CoV-2 viral strains. Luckily there is a quick and cheap way to find these strains if they exist – test asymptomatic/mild case swab samples for COVID-19 and then genome sequence the SARS-CoV-2 strain that has infected them with the aim of identifying a virus with mutation(s) in essential viral gene(s). This is what the Chinese researchers did to find their less pathogenic strains and how the Singaporean researchers found their deletion mutant strain.
This approach is cheap (a couple of hundreds of dollars per virus strain) and quick (a week or less). With little cost we could sequence a few thousand viral strains, or even tens of thousands of strains, from positive swab sample from asymptomatic and/or mild case until we find a virus strain with the right mutations to make it harmless and which could work like a vaccine to protect us from the dangerous strains. We would know from epidemiology that this strain can still reproduce in people and lead to immunity, but not make people seriously ill.
Update. I have written a step-by-step post on one way we might go about putting this proposal into action.
What viral mutations are we looking for in a good non-pathogenic viral strain?
We would ideally be looking for a virus strain with a large(ish) deletion in an essential viral gene like the strain found in Singapore (unfortunately this strain is too dangerous to use as it put people into hospital). This sort of deletion mutation is easy to spot in the SARS-CoV-2 genome data, and because the genetic information has been removed, it makes the virus unlikely to be able to mutate back into a dangerous strain. Ideally, the strain identified will have infected a large number of other people in the local area so we can know it is safe from the epidemiological data. This will be important for getting regulatory approval to use the strain.
Has this ever been done before?
Yes. The polio, measles, rubella, mumps, and chickenpox vaccines are all live attenuated viruses. Even something as dangerous as smallpox was controlled in the 18th century using a variation of this idea called Variolation. The idea was the doctor would deliberately infect you with a less harmful strain of smallpox (often at a low dose) to make you immune to the more deadly strains of smallpox. Of course, they didn’t know how this approach worked in the 18th century, but it was still very effective and millions of people were saved from dying from smallpox by it.
Some people have been calling using a low dose of the virus Variolation, this is not what we think Variolation was, but this is a complex topic. While such a low-dose approach of the dangerous strain might make the COVID-19 less dangerous to the person being deliberately infected, it doesn’t make the virus any less dangerous for those around you that you might infect later. Such an approach could also not be used on the vulnerable, leaving them exposed to the illness. There is no reason in principle that the low dose idea couldn’t be combined with the attenuated strain idea and it might even be a very good idea.
In regards Corona viruses, there was considerable work done on determining which regions of the SARS-CoV can be deleted to create an attenuated virus that provided protection from the wild type dangerous version. Jose Regla-Nava and colleagues identified that SARS strains with gene deletions in the E protein were attenuated and provided good protection from later infection with SARS-CoV. Furthermore, these researchers found the deletion strains were genetically stable when grown in cell culture. SARS-CoV-2 contains the same E protein and deletions in the E protein gene may provide the same attenuation.
What are the risks?
The major risk is a mutant virus we think is safe is not 100% safe. While we can use community spread of the identified strain to estimate how safe it will be (i.e. if it has infected 1000 people and none have got seriously ill then we should have a pretty good idea that it is safe), our knowledge will be incomplete. We can of course spend the next few years testing and trialling, but if we do this by the time any strain is shown to be 99.99% safe (not even the polio vaccine is 100% safe) we will have all got COVID-19 and the world’s economy will be a smoking ruin.
We have a choice of taking some risks now, or face the certainty of a much worse problem later. Time to accept some risk and do something now.
Q & A
I have been getting a few questions on this post so I thought I would address them here.
How do you know there is an attenuated viral strain out there?
Because such strains have already been found. I am hypothesising that there is more than one based on the known mutation rate of coronaviruses and the number of cases. Coronaviruses like SARS-COV-2 mutate continuously (this is why companies like deCODE can tell the geographical origin of different strains) as the molecular machinery for replicating their RNA genome is not very accurate, although it is more accurate than the machinery of other RNA viruses like HIV. When you combine this with the millions of mild cases out in the world, the odds are on our side that there is at least one person infected with a strain that has a mutation that makes the virus less dangerous (attenuated). We just need to go and look for this strain – luckily the tools we need to use (genome sequencing) are now cheap and quick. What would have been impossible 20 years ago can now be done in a week.
Aren’t most people who have mild/asymptomatic cases infected with a dangerous strain?
Yes. Almost all people (>99.9%) who are infected (and have a mild case) are infected with a dangerous strain of the virus, they just happen to have an immune system that can control the virus well. With COVID-19 a mild case does not mean you are infected with an attenuated strain – for most people with a mild case if they happen to infect a person with preexisting conditions or who is old, that person will be at a high risk of dying. A mild case does not equal a harmless strain.
My argument is coming from the other direction. While almost all mild cases of COVID-19 are caused by a dangerous strain of SARS-CoV-2, an attenuated strain of SARS-CoV-2 will only cause mild disease. If you want to find an attenuated strain you need to look at mild cases even though >99.9% of the people you check will be infected with a dangerous strain. What we want to find is one of the rare natural viral mutants that has a mutation that makes it attenuated. Where you will find such a viral mutant is in people with the mild/asymptomatic form of the disease.
I am NOT arguing that people with mild cases are infected with a mild strain of the virus. If this is what you think I am saying please take the time to read carefully what I have written – yes it might sound like this is what I am saying from a five second scan, but this is not the case.
Why only sequence those with mild/asymptomatic cases of COVID-19 in the search stage?
If I had to choose one aspect that gets most misunderstood by people who read this idea, it would be the reason for sequencing only mild/asymptomatic cases. This choice is purely an efficiency issue. In an ideal world we would sequence the strains from every case in the world, look to see if we can find mutants with deletions, and then check what was the clinical outcome of those infected with each strain was. If we find that all clinical cases of a particular mutant strain are mild/asymptomatic, and no cases ended up in hospital, then we would have our candidate strain.
Unfortunately we live in a constrained world where it is not possible to collect and sequence the virus from every case of COVID-19, Given this, where should we look first? Since we are looking for a mutant strain that only causes mild/asymptomatic cases, we can exclude patients in the first pass who have serious symptoms. Any strain that causes serious illness won’t be a strain we want to use.
It is only once we find a good candidate attenuation strain that has the right sort of mutation (a deletion) that we then collect swab samples and sequence all cases in the local area. At this point we will need to look at both the serious and mild cases (include everyone in the local hospitals), to get the full clinical picture of the strain. This approach of initially screening just the mild cases is a simple way to make the search process for an attenuated strain more efficient and practicable.
Can’t we just wait for a COVID-19 vaccine?
No. Apart from the time it will take to develop, trial, and mass produce a vaccine (12-18 months), it is unlikely that any vaccine will be practicable. The reason why is immunity to respiratory viruses (like corona) doesn’t last long – 6 months to 2 years. We would have to keep vaccinating everyone in the world every year (or maybe every 6 months if we are unlucky). This just isn’t going to work in the real world (especially poor countries) and is one of the reasons we don’t have a vaccine for the coronavirus strains that cause the common cold. Unless we can drive the current dangerous SARS-CoV-2 strains to extinction we are going to have a problem with this disease indefinitely.
Update. A very interesting pre-print has been released on the natural immune response to SARS-CoV-2. Many people don’t develop much of an initial immune response (IgM antibodies) and the long term immune response (IgG antibodies) fades quickly after just two months (see figure below). While this is more of an issue for those people arguing that we should lift social isolation restrictions to allow the population to develop herd immunity (this would just kill a lot of people and any herd immunity would quickly disappear), it is also a concern for any vaccine approach that can’t drive the dangerous strain to extinction (i.e. all the other conventional vaccine proposals). 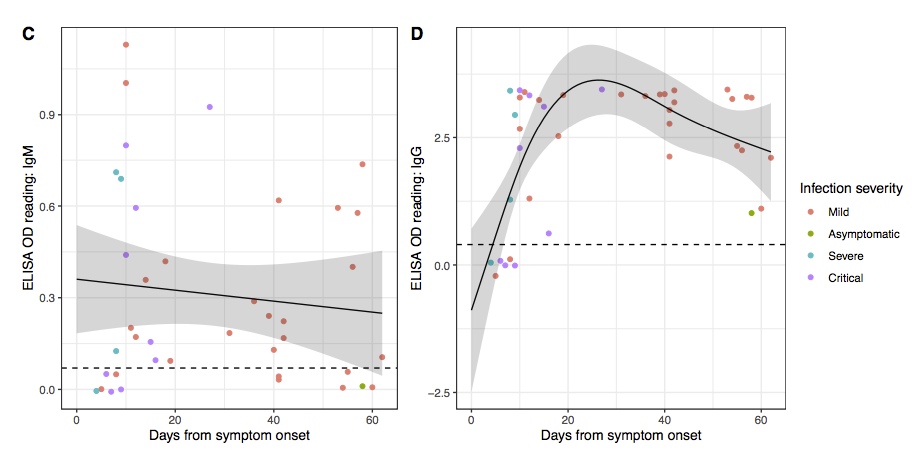
Won’t the mutations in SARS-CoV-2 make this proposal fail?
The coronavirus are relatively stable genetically for an RNA virus. The coronavirus strains that cause the common cold tend to not change much antigenically over time, unlike the Influenza, HIV and Hepatitis C viruses. The way the common cold strains spread is through our immunity to them declining fairly rapidly (in months, not years). The result is the same common cold strain can infect you multiple times in your life as your immunity to it fades, rather than it having to change antigenically so much that our immune systems doesn’t protect us anymore.
This is good news as it means we may only need to isolate one mutant strain. Even if in the worse case SARS-CoV-2 does change so much antigenically that our attenuated strain no longer offers protection, we can just repeat the process we used to find the first strain to find the next strain. More fundamentally, this is a problem for all vaccine approaches that we will need to deal with if it happens, but it shouldn’t stop us from acting now.
Update. A recent non-human primate study out of China using a conventional vaccine approach found that the antibodies produced were neutralising for all strains found around the world. It really does look like we only need only one attenuated strain to provide protection for all strains.
Isn’t social distancing and quarantining solving the problem?
Yes and no. Yes countries like South Korea and Australia have shown that through mass screening and social distancing you can keep a lid on the disease, but this leaves the population susceptible to a new outbreak. Singapore and Japan have recently seen this in action where they eased restrictions and found the disease came back and they had to reintroduce restrictions. I don’t think many people want to live for years with cycles of restrictions, easings and further outbreaks.
Wouldn’t the use of such an attenuated strain just be a vaccine?
Yes in one way, but it is a little more subtle. Assuming we can find an attenuated strain, then how to best use it a separate question. The most important thing to note is that a natural attenuated virus is not a vaccine. It is just a natural virus that you can catch in a natural way. Hang out with someone infected with the attenuated strain and you will catch it without doing anything, go home and those around you will catch it from you, and so on. While I wouldn’t suggest this is the best way to get an attenuated virus out into the community, such natural spread is outside the regulatory framework for vaccines.
Of course the use of a natural attenuated strain as a vaccine would fall under the regulations for vaccines, but the mere existence of an attenuated virus does not make it a vaccine. Each regulatory authority around the world would need to weigh the evidence of safety (obtained from the epidemiology) against the risks. Some regulatory agencies may decide the rewards from using such a strain as a vaccine is worth the risk, while others may decide they are not.
What effect would using an attenuated SARS-CoV-2 strain have on the dangerous strains?
Giving a natural attenuated viral strain deliberately to lots of people would change the ecosystem for the dangerous strains of the virus. The dangerous strains would find it difficult to spread through the community as many (most) people would have already been infected (and hence immune) with the attenuated strain (i.e. have herd immunity). Overtime the dangerous strains would become rarer, and the attenuated strains more common, until eventually the dangerous strains would become extinct and we would just be left with the mild version floating around. While we would not be able to get rid of this mild strain, it would just be another of the hundreds of viruses out there causing common colds. This proposal at its base is really one of replacing the dangerous strains with a less dangerous strain that we can live with.
It is the ecology aspect of this proposal that makes it different to other attenuated vaccine proposals. Currently all attenuated vaccines developed in the lab are designed to just protect the person receiving the vaccine. An attenuated strain identified by screening infected people (epidemiology) will identify a strain that can still be transmitted from individual to individual. This makes the use of such a strain radically different than a conventional lab created attenuated viral vaccine.
Why can’t we just use the less pathogenic SARS-CoV-2 strain already identified in China?
While the ZJ01 SARS-CoV-2 strain identified in China appears to be less pathogenic, the mutations that make it so are single base changes. These can easily mutate back to the more dangerous version of the virus. The viral strain we want to find will have a deletion mutation where a section of the viral genome is removed. Deletion mutations are much more difficult to mutate back to the dangerous type since rather than just a change from one nucleotide to another (e.g. C > T), the deleted region is missing and can’t easily be recreated by mutation. Put simply, deletion mutations are more stable to back reversion.
How should any natural attenuated SARS-CoV-2 strain be used?
This is not a decision for me. I think the regulatory authorities like the FDA will approve the use of a natural attenuated strain on the basis of the epidemiological data collected finding the strain that show it is safe. While most regulatory agencies are extremely conservative and slow, they are not idiots and they understand that using an approach with some serious unknowns might be better than the alternative of waiting for the perfect vaccine. COVID-19 is a problem with only hard choices.
I do think it would be impossible to prevent the use of any such strain even without regulatory approval. Assuming a natural “safe” strain is found and a test for it developed (this is relatively easy since you are looking for the presence of a deletion), people will start spreading it between themselves at a “grass roots” level. I think this outcome will influence the decision of the regulatory authorities to approve its use – better to have the attenuated virus spread in some controlled and regulated way, rather than illicitly by people doing it on their own. Just to make clear, I am not suggesting that it is a good idea to allow “grass roots” spread (I think it is a bad idea), nor am I advocating for it, just that I think it won’t be possible to stop such spread if the regulatory authorities don’t license it.
Even if you think a natural attenuated strain is too dangerous to use as a vaccine directly, it would be extremely useful to speed up other vaccine approaches. One way it could be used is to give it as a challenge to volunteers who have received another vaccine to see if the vaccine provides protection without putting them at risk. Knowing if a vaccine works (i.e. provides protection from the disease) is one of slowest steps in new vaccine development. If you are going to do a viral challenge with SARS-CoV-2, you really want to use a strain you know is harmless, rather than one you know could kill your volunteers. Of course to do this you first have to make the effort to find such a harmless strain.
I have objection X which means this whole idea is worthless!
If you are not a scientist then I will be blunt and say it is almost certain that your objection is either wrong or irrelevant (sorry for being harsh). While I have presented the idea in as non-technical way as is possible, it is still a complex scientific idea with many complex parts. What might seem to you a very strong argument is likely to not hold up when explored in depth.
If you are a scientist try not to get caught up too much in me skipping over certain technical details and instead focus on the bigger picture. This is a proposal for an approach that may work, not a grant application where all the experiments have already been done. There is a non-trivial chance that this approach may not work. I am aware of this, so I ask you to please focus not on all the possible ways it may not work, but if there is anything that will make it certain to not work. If there is some fatal flaw then please let me know, not that step x might not be easy, or we don’t know some particular fact. This is a problem where assumptions have to be made and risks taken.
It is not ethical to use such a natural attenuated strain!
This is a proposal to search for a natural attenuated viral strain of SARS-CoV-2, not an proposal to use such a strain. Finding such a strain does not mean we have to use it, just that we can use it. Ultimately the decision to use such a strain will be a political and social question weighing up up all risks, but we can only have this debate if we make the effort to find such a strain and show it is safe.
If you think that the whole idea is unethical under all circumstances, it is worth keeping in mind that it exactly the same as what Sabin did with the oral polio vaccine. He found a natural attenuated polio strain in a child with a mild case of the disease and used it in his vaccine. His vaccine has gone on to prevent tens of millions of cases of polio. Yes there was and still are risk with his vaccine, but most people think it was huge step forward for humanity.
How would this search work in practice?
I have written a second post describing how we might go about turning this idea into reality – How would a search for a natural attenuated SARS-CoV-2 strain work in practice?
Update. I have been trying to get this idea in front of someone with the clout to make this happen, but without much luck because the people with the clout (say Bill Gates) don’t read messages from random people like me. For this idea to succeed it needs a two hop process (i.e. someone knows someone, who knows someone, who Bill Gates will take seriously). If you think you might be that first hop person then please get in contact with me at daniel.tillett@gmail.com.
I should add that it doesn’t have to be Bill Gates that can push this forward. If you think you know someone who could help then get in contact with me. Unlike Bill I will respond to your email :)
Update 2. I have modified this post to better explain those aspects that have confused people (my fault). I hope this idea is now clearer. Keep the comments coming and if you think someone you know would be interested then pass the post along along.
Update 3. This is directed at my fellow scientists. If you happen to working on this exact idea please get in contact me – not least so I can give you lots of money to speed up your work.
Update 4. This field is moving at an amazing pace with new results coming out every day. I have updated this post with the most relevant new data.
No I haven’t. If you can get his attention then please raise it with him.
This is a complex topic. I have updated the post to make this clearer. The major problem is we really don’t know how exactly variolation as done. We do know that many practitioners used pox material from patients with mild strains, and we do know there was pathogenicity variation in the smallpox strains circulating. I suspect variolation worked through using both low doses and low pathogenicity strains, but this is hard to now determine. It may well be using both an attenuated strain of SARS-CoV-2 and a low dose strategy is the way to go.
This is complex – 50% are asymptomatic at testing, but many go onto develop mild symptoms. I have updated the post to make this clearer, but it is not too important.
Sort of, it is much more similar to variolation which proceeded vaccination with cowpox.
No I wasn’t aware of this. I will send him an email now. Thanks.
While I can afford to do the initial work myself I can’t get the samples and more importantly I don’t have the political clout to do the secondary screening in the local area once a strain is found.
Well this is a topic that should probably be raised on that topic. I have noticed that the masses seem to have lost interest in Bitcoin after the crash in price.
Thanks. Fixed.
Would it be good idea then to make “friends” with someone who is Corona Virus positive, similar age and health, but asymptomatic to see if I can catch that strain first rather than the deadly strain?
Or is that being simplistic and reckless?
Humour: Maybe we could have Corona bars/parties for self infection/inoculation? I think they would be popular.
PS Are the tests that accurate that asymptomatic infections are not false positives?
It would be a very bad idea since almost all people with a mild or asymptomatic case of COVID-19 are infected with the common deadly strain.
There are quite a few false positives it appears from the tests. The PCR based test is very sensitive.
There have been reports on the news that people who have been infected with CV are being infected again or has the virus re-erupted?
Would this support your idea of separate strains, like common cold, but also work against your idea of “immunisation” through live, low virulence inoculations?
Secondly has not most of the “anti-vaxxers” PR war been based on the results of using active viruses for vaccinations? Is there a real risk in this day and age that any slip up will be seized upon by these hysterical people and further inhibit any realistic progress. FB and all the other social media tentacles raise the bar even higher for testing. (Mind I am sure not many of them were rushing off to Italy with not needing vaccinations to help out).
Thank you for such a level headed and thought provoking article. Much appreciated.
Rob
No one knows at this stage in regards if it is people getting reinfected, or if these as false positives, or if the virus never went away fully. This is something we need more research on.
As for anti-vaxxers who knows. We can safely ignore them for now.
Hi Daniel,
Thanks to HackerNews, I read your article on a possible solution for COVID-19 and also your plea for help.
I have tried to connect you with Bill Gates using my membership of Gates Insider.
Also I have written an e-mail to Dr. Stephen Wolfram and copied you on CC.
Those are my 2 cents of contribution to your quest to find a cure for COVID-2019. :-)
Please check the comments section of https://www.gatesnotes.com/Health/What-our-leaders-can-do-now
Thanks Sunil. Let’s hope something comes out of this.
Sounds good. But Bill Gates wants to profit from a vaccine. He’s not the right person to ask. This should be out in the public domain and disseminated throughout the relevant scientific community, and pressure must be brought to bear on governments.
I doubt that Bill is looking to profit from a vaccine, but this doesn’t have to be driven forward by Bill. The only requirement is the person or group driving this forward has the political clout to make it happen.
If we understand what makes a deadly virus less deadly, can we not engineer the less deadly version ourselves rather than searching for it?
Sure if we knew what makes a deadly virus less deadly which we don’t. This is why we are using nature to do the experiment for us.
Could we use a low dose of the regular (dangerous) strain to trigger an immune response in healthy people if they then followed a two week quarantine? I understand that an asymptomatic person still spreads, but if the infection was done intentionally at a low dose and followed by a quarantine, would this not help build herd immunity? (Also helping coordinate things like work time off.)
Amazing article! Just wondering: since what you’ve described is apparently a well-known technique, why do you think others have not pursued it? Are there perhaps some complications you may not be aware of? Or perhaps biotech companies are currently working on it? Also, aside from any economIc factors, how much more dangerous, if at all, is your approach vs waiting for a traditional vaccine? Can you attempt to quantify that in terms of deaths? Thanks!
The is the low dose approach that Robin Hanson is promoting. I suspect it would work, but it has some limitations that I think would make it less desirable in the real world, not least trying to get regulatory approval to run the experiments. As I mention in the post there is no reason you couldn’t combine a low dose approach with an attenuated virus – it might very well for vulnerable people.
No idea. It is possible that I am the first person to have thought of it – it seems unlikely, but nobody so far has got in contact with me and said they are working on it.
My approach is not dangerous at all since it is just a search for a virus that hopefully is already out there. Of course using it may be dangerous, but that is not a decision for me to make. Personally I would be willing to take a few more risks because of the consequences of not having a vaccine (especially on poor countries), but this is just my personal opinion. There are no easy choice with this disease.
Hi,
you focus all around the assumption that different responses comes from different virus sequences.
but what about the human heterogeneity is the cause of a different response (mild asymptomatic, severe, etc), very much similarly to an allergic reaction?
In the end the human-to-human diversity in the immune system can be quite overwhelming compared to the few differences in the 30kb genome of covid19.
Cheers,
antoine
I know this is probably a long shot but you could try to call 2GB radio & speak to Alan Jones or Ray Hadley? They might help you find someone, who knows someone to move this idea forward.
*Just a random thought*
“be killing between 1% to 3.5% of the people we know it infects (i.e the case fatality rate)”
Should be killing between 1% to 3.5% of the people diagnosed with COVID-19 (mostly serious cases who get into the hospital)
Hi, I’m planning to write an article about this in a major Brazilian newspaper, and had a few questions.
I can contact you by email, but thought it might be better to leave your answers here, so that they can be perused by other interested parties.
The first questions is: how do we identify harmless strains, and how reliable is this method of identification?
Is it reliable enough that regulating agencies might forego the need to run it through the multiple testing phases for vaccines (before wide-ranging distribution throughout the population)?
Thanks,
Henrique
I have a question: Why does the attenuated strain have to be *natural*? How about, we artificially delete some parts of the genetic sequence of an arbitrary (dangerous) strain in the laboratory based on some educated guess, and test this articially altered strain for the results? How would you compare this approach in terms of efficiency and risks to looking for an attenuated strain “in the wild”?
It only has to be natural because it will take a long to get to the point of testing in humans an artificial deletion strain. We can use what nature to run the experiments that we just can’t run we a lab created strain.
I specifically say that the difference in clinical outcome in >99.9% people is due to the individual person. This is not what this idea is about.
Australia is really a bad place to try and do this work as we have so few cases (so far). This really needs to be done in Europe or North America where the cases are.
The “we know it infects” are the cases that have been diagnosed. Probably the best place to check on the true death number is South Korea as they have done a pretty good job of contact tracing all cases to find asymptomatic and mild infections. In South Korea the death rate is near 2% of the confirmed cases.
Henrique it would be best to contact me by email.
I am currently writing a new post on answering exactly your questions on how this idea can be put into practice. If we do this work well then I think the regulatory agencies will fast track the approval on the basis of the epidemiological data gathered, but ultimately this is a question for the regulatory authorites.
This is a great idea and it deserves to be pursued.
I’m worried concluding safety based on epidemiology may be difficult. The case mortality rate is far from uniform across demographics. Not only age, but existing health problems contribute to morbidity and mortality.
So, for a strain to be considered “mild” based on just observation, enough vunerable people need to contract it and recover without complications. Additionally, since this virus is so contagious, regulators will likely not be satisfied with flu-like mortality of 0.1%.
So we’ll need a minimum of 10k naturally occurring confirmed cases of the mild strain in relatively vunerable people, which is not beyond the realm of possibility, but I worry it will be very difficult to track down so many cases (assuming the mild strain is rare).
It is hard to know a priori what the regulators will accept after a few more months of social isolation.
Yes there will be risks involved with using an attenuated strain where safety has been established via epidemiology, but there are also risks with not using such a strain. This is a problem where waiting for the perfect safe solution will come at great cost. It all comes down to balancing risks.
Germany has 6 times less death than other European countries, could it be related to a safer strain of the coronavirus due to a mutation? Or is it all due to the extensive testing of people in contact with someone who is sick?
Impossible to know until this is actually looked into, but I think it more likely due to Germany being better at testing. Many countries in Europe are only testing people who are sick in hospital with COVID-19 symptoms.
This is by far the most intelligent promising idea I’ve read thus far.
Just FYI, I’ve blogged your proposal and privately run it by a few people.
https://irfankhawajaphilosopher.com/2020/04/12/daniel-tilletts-attenuated-sars-cov-2-strain-proposal/
For whatever it’s worth, initial response has been positive. Just a tiny contribution to the overall effort you’ve begun.
Please look at the brilliant former NASA engineer/now super popular science vlogger Mark Rober. He did one of his videos with his good friend Bill Gates and you can leave comments below on his YouTube page, so you could forward your info. to him! I think you’ll also find his educational science videos light-hearted yet extremely entertaining. Best of luck to you!
Have you tried contacting Kári Stefánsson of deCODE genetics in Iceland (https://www.decode.com/management/)?
They seem uniquely posed to do this, based on having sequenced all the infections found on Iceland.
During the Asian Flu, America developed and distributed a vaccine in several months and it was pivotal in stopping the flu from spreading to more people and eventually ending it.
Do you think the world could find and bring forth a vaccine in similar succession for SARS-CoV-2?
https://daily.jstor.org/how-america-brought-the-1957-influenza-pandemic-to-a-halt/
Hi Daniel,
Thanks for the nice article. My question is if people know about the E-protein that you mentioned, is there any progress made on that front?
There are two major difference from 1957:
1. We had a vaccine for influenza that was designed to be adapted to a new strain quickly.
2. The regulators and more importantly scientists and doctors were used to the idea of moving quickly and taking risk. We seem to have lost this and now want 100% certainty with everything even when faced with serious problems that require fast action.
Not that I know of. The lack of thinking down this path is hard to fathom.
Hi Daniel,
I’m in the UK. I am 68. I am a golfer, and I know of people my age who were very ill in Jan/Feb with a weird flu like bug. Would it not be a good idea to selectively advertise for folk, say over say 65, who thought they might have had it, and had got through it? I think with that approach that you could find you milder version quite quickly. Just a thought. I like your approach! Thanks
Shaun yes it would be worthwhile looking at those over 65 with mild cases, but to isolate the virus you need to have not already had it sometime ago. If you were ill in Jan/Feb then the virus is long gone from your body and so we can’t isolated the virus anymore.
Daniel,I like your thinking. Have you contacted Michael T Osterholm author of
“Deadliest Enemy our fight against killer Germs” He is listed as still working at the U of Minnesota
Seems like he has developed lots of contacts over the years including influential ones
If I’m reading this right, are you effectively suggesting the use of a “contagious vaccine”? Wouldn’t all the issues the make vaccine testing take so long (evulating side effects, effectiveness, length of immunity, and so on) be even *more* important for a vaccine that spreads non-consensually throughout the community?
I am not suggesting the use of anything, I am suggesting we look for such a strain. What is done with such a strain is not for me to decide.
If we do find such a strain it is already spreading in the community on its own with any testing or consent. If this is happening then we should study how it behaves and then decide if we want to use such a strain weighing the risks and rewards. Outside of using such a strain directly as a vaccine, it would be extremely useful to use under highly controlled conditions to test other vaccines approaches. I talk more about this is this post
It is unethical to not search for an attenuated SARS-CoV-2 strain